Thoracic Stabilization
- Home
- Thoracic Stabilization
Thoracic Stabilization
Introduction
Like any other bone, the spine can also be the seat of infections, both pyogenic or tubercular. Spinal tuberculosis is the most common site of bony tuberculosis. Several vertebrae can be rapidly destroyed leading to a collapse of the bony structure and an unsightly ‘Hunch Back’ deformity. Children are especially more prone for developing the deformity as the deformity can continue to progress even after the disease has been cured. This can subsequently lead to severe compression and stretching of the spinal cord with resultant paralysis of both the lower limbs.
In the early stages of the disease, use of anti-tubercular drugs is sufficient for complete cure. However, in severe cases and in patients who have weakness or paralysis of legs, surgical decompression of the spinal cord along with medication becomes an important consideration. Surgery removes the pressure effect on spinal cord, prevents progressive deformity and gives good relief of pain. Implants made of specialized metals and bone grafts are used stabilize the spine while the healing process ensues.
What causes spinal tuberculosis?
Spinal tuberculosis is caused by Mycobacterium tuberculosis. Infection results from hematogenous dissemination from a primary focus, usually the lungs, although associated active focus is identified in only less than 10%. The most common site of infection is the paradisical type, where two adjacent bones on either side of a disc are commonly involved
What are the symptoms?
Back pain associated with restriction of movements of the spine is the usual presenting feature. Constitutional symptoms of malaise, loss of appetite and weight, evening rise of temperature and night sweats are also common but can be absent in patients with good nutrition.
As the disease progresses, collapse of the spine is evident with prominence of the spinous process as a sharp deformity in the early stages and a very prominent deformity (kyphosis) in late stages.
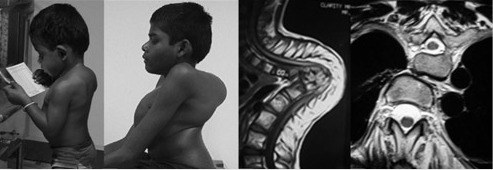
Clinical photographs of a child affected by spinal tuberculosis at the age of 4 years. Though the deformity looks minimal at the completion of chemotherapy, it has significantly worsened by adolescence. MRI image shows a buckling collapse with cord compression.
Tuberculosis can present with huge abscess formation. This is called a cold abscess due to lack of high grade fever and warmth and may be clinically evident in the back.

Huge bilateral psoas abscess in a patient with thoracolumbar tuberculosis. The anteroposterior radiograph shows paraspinal soft tissue widening due to the abscess which is confirmed in the axial MR images
The pus and the bending deformity can cause pressure on the spinal cord resulting various grades of paralysis. Neurological involvement initially presents as in-coordination, clumsiness while walking and slowly progresses to paralysis.
What are the standard investigations?
In the blood tests, erythrocyte sedimentation rate may be markedly elevated (> 70 mm/ hr), and serial ESR measurements also help in assessing the response to treatment. The white cell counts is raised with particular raise in the lymphocytes.
Xrays show bony destruction and deformity. CT is useful in assessing accurately the extent of bony destruction, early identification of posterior element involvement, and in tuberculosis of specific sites like the craniovertebral and cervicodorsal junction, the sacro-iliac joints and the sacrum. MRI is the gold standard for demonstrating the extension of disease into soft tissues and the spread of tuberculous abcess. MRI is the most effective method for demonstrating spinal cord compression. The diagnosis is confirmed by histopathological (“biopsy”) examination of the infected tissue.
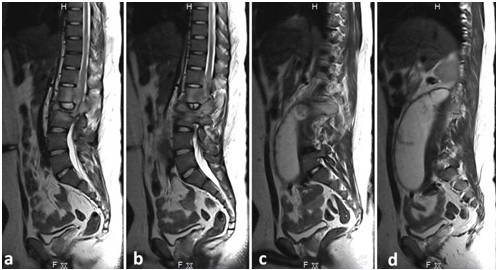
The tracking of a psoas abscess shown through serial sagittal images. The abscess that develops in the disc and adjacent vertebral body (a), tracks along the neural foramen and the psoas sheath (b,c), and forms a huge paravertebral psoas abscess.
What is the treatment?
General supportive measures include bed rest, external bracing, nutritious diet, vitamins as required, care of bladder, bowels and good nursing care. Modern anti-tubercular drugs are able to achieve excellent clinical cure. Hence spinal TB is considered as a medical disease with selected surgical indications. Multidrug chemotherapy is administered for all the patients and bed rest with external bracing is advised in the initial period. The patient is followed carefully till complete healing. Surgical treatment is recommended for certain specific indications like extensive neurological deficit, severe pain, instability, deformity of the spine and lack of expected response to medications. The currently recommended first line drug regime is four-drug therapy. This includes Isoniazid 5 mg/kg, Rifampicin 10 mg/kg, Pyrazinamide 20 – 25 mg/kg, and Ethambutol 15 mg/kg for two to three months followed by Isoniazid and Rifampicin for four to six months. The aims of surgery in spinal tuberculosis are to obtain tissue sample for biopsy, drain an abscess cavity, achieve debridement of disease focus and to stabilise the spine.
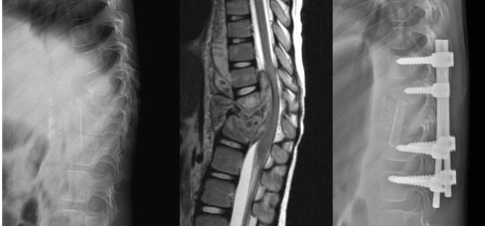
Thoracolumbar tuberculosis in a child with destruction and huge abscess causing cord compression. The lesion has been treated by anterior debridement with fibular strut graft reconstruction and posterior pedicle screw stabilization.
Surgical Expertise
Testimonials
What Our Patients Say
EXCELLENT rating
Based on 107 reviews My father had rotator cuff problems and needed follow-up care.Dr.Ankith N V was exceptional. They provided thorough, compassionate care and clear communication. The clinic was well-equipped, and attentive Highly recommend.
My father had rotator cuff problems and needed follow-up care.Dr.Ankith N V was exceptional. They provided thorough, compassionate care and clear communication. The clinic was well-equipped, and attentive Highly recommend. RAVINDRA KUMAR2024-06-09Very good Orthopaedic Clinic and Dr Ankith sir well experienced Dr and also clear all the doubts for patients and their families...
RAVINDRA KUMAR2024-06-09Very good Orthopaedic Clinic and Dr Ankith sir well experienced Dr and also clear all the doubts for patients and their families... Dilip Gowda BR2024-05-29I had an outstanding experience with Dr. Ankit at Ankit’s Orthopedic . Dr. Ankit’s exceptional friendliness and professionalism made me feel comfortable and well-cared for throughout my visit. I highly recommend Dr. Ankit for their exemplary patient care and welcoming demeanor.
Dilip Gowda BR2024-05-29I had an outstanding experience with Dr. Ankit at Ankit’s Orthopedic . Dr. Ankit’s exceptional friendliness and professionalism made me feel comfortable and well-cared for throughout my visit. I highly recommend Dr. Ankit for their exemplary patient care and welcoming demeanor. Nikhil L2024-05-29Doctor is so knowledgeable and humble. Also he listens to us keenly and understands the problem. Highly recommended.
Nikhil L2024-05-29Doctor is so knowledgeable and humble. Also he listens to us keenly and understands the problem. Highly recommended. Akshay2024-05-29Good communicate with patients and cooperation well good, we are satisfied your treatment.
Akshay2024-05-29Good communicate with patients and cooperation well good, we are satisfied your treatment. renuka Mallikarjuna2024-05-22Best orthopaedic clinic in vijayanagar good service
renuka Mallikarjuna2024-05-22Best orthopaedic clinic in vijayanagar good service ಬಳ್ಳಾರಿ ನಾಗ2024-05-22Very good doctor and
ಬಳ್ಳಾರಿ ನಾಗ2024-05-22Very good doctor and Kiran S2024-05-18Really...this clinic is too good i recommended Dr.Ankith sir ..and doctor treat very well, he had more knowledge and as well as good human being and his staff is wonderful, this is the perfect place for orthopedic and spine
Kiran S2024-05-18Really...this clinic is too good i recommended Dr.Ankith sir ..and doctor treat very well, he had more knowledge and as well as good human being and his staff is wonderful, this is the perfect place for orthopedic and spine ashoka vc2024-05-17Good service well qualified doctor
ashoka vc2024-05-17Good service well qualified doctor srinath v2024-05-17
srinath v2024-05-17
Book Your Appointment Today!
Call us at 099644 83761 to schedule your visit. Your path to recovery begins at Dr. Ankith’s Orthopedic & Spine Care Clinic. We look forward to helping you achieve your health goals!